A GP marketplace built from inside an industry that needed a better way.
After a decade placing GPs across Australia, I kept asking the same question: why does it cost a clinic $20,000 to find one doctor — and who’s really paying that price?
- $20k
- typical placement fee
- A decade
- placing GPs
- Direct
- clinic to GP

That $20,000 fee comes from somewhere.
 01
01A system built on commission, not fit.
After nearly a decade inside the Australian GP recruitment industry, I’d watched the same cycle play out hundreds of times. A clinic needs a GP. They call an agency. The agency headhunts, vets, pushes paperwork, and delivers a shortlist — often with a commercial incentive toward whoever pays the most commission, not necessarily whoever is the best fit. The invoice arrives. $20,000 for a single doctor.
Someone always pays — and it’s not the agency.
That fee has to come from somewhere. Sometimes it’s the doctor, whose offer is quietly shaped by what the agency needs to earn. Sometimes it’s the clinic, cutting admin costs or consumables to stay afloat — and those cuts ripple outward.
At the end of that chain is a patient, whose favourite doctor moved on because the support wasn’t there. Or who turns up to find there’s no face mask available because the clinic can’t absorb another overhead.
 02
02The patient carries the weight
of a system they never chose.
“Clinics and GPs work incredibly hard to provide exceptional patient care. The fee itself isn’t the problem — it’s what the system underneath it costs everyone who never sees the invoice.”

The ripple effect on patients — and communities
GPs don’t make career decisions the way other professionals do. They have patients’ lives on their shoulders. One wrong placement — a clinic with misleading billing structures, inadequate admin support, or a culture that doesn’t allow quality care — can affect a doctor’s ability to practice. It can put their AHPRA registration at risk, drive up their indemnity insurance costs, or push them out of the workforce entirely.
In a country already facing a GP shortage, every doctor who leaves a role they weren’t properly informed about is a community left without care.
I built Heart Bridge Health because that mattered to me — not just commercially, but personally.
I found a way to make it make sense.
Every part of the agency fee exists for a reason — headhunting, vetting, paperwork, compliance, the pitch. Heart Bridge Health doesn’t pretend those needs don’t exist. It builds the tools to meet them directly, between the people who matter most.

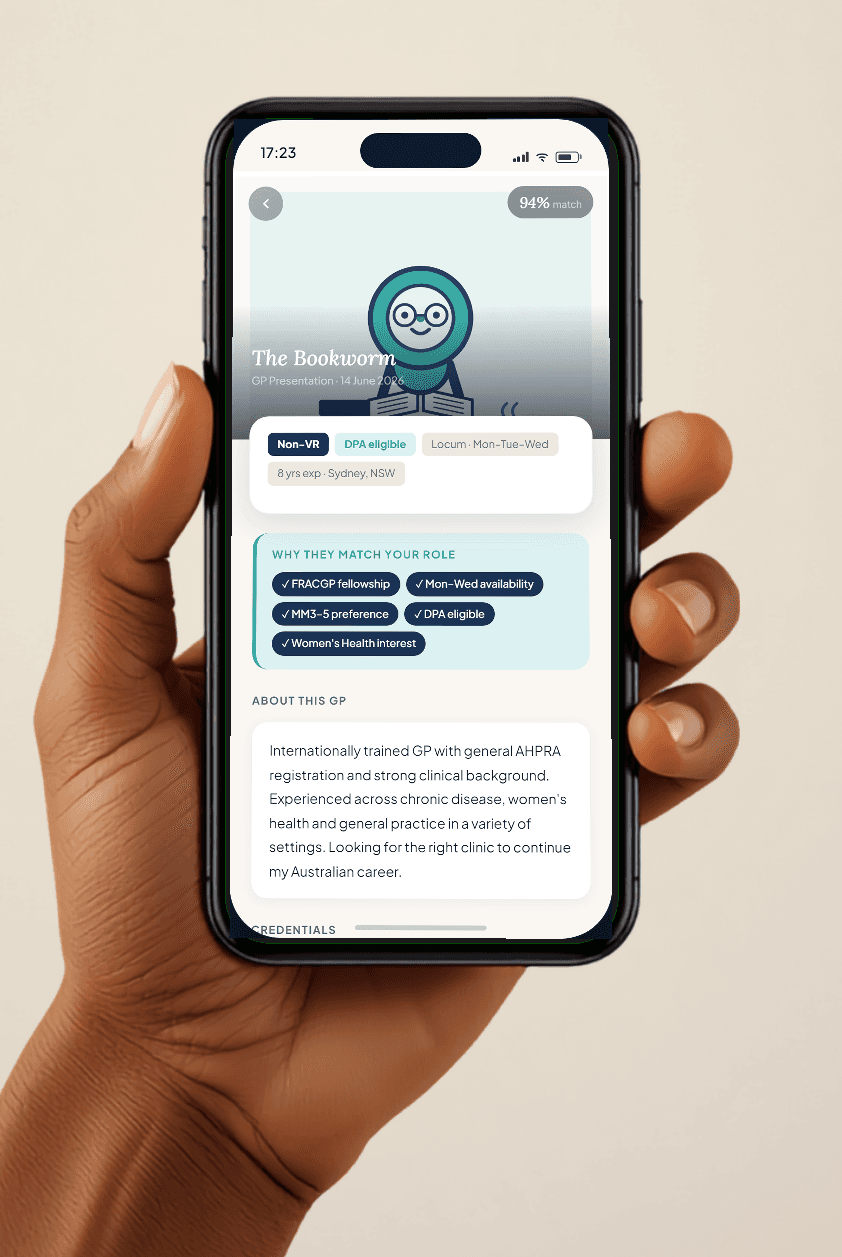
Smart matching — vetting built in
GPs only see opportunities they’re actually eligible for. DPA classifications, fellowship requirements, visa conditions — the platform does the filtering before anyone wastes time on a role that was never going to work.

Direct communication — no middleman
Clinics and GPs talk to each other from day one. No agency shaping expectations in either direction. What you say is what they hear — honest connections from the first message.
Lumi AI — compliance without the consultant
Lumi handles the complex questions — DPA compliance, Medicare billing rules, contractor terms, AHPRA pathways — 24/7. The guidance that used to require a phone call to an agency is now instant, accurate, and free.

Hearts rating — trust that goes both ways
Two-sided reviews after every placement. GPs know the clinic's culture before arrival. Clinics attract doctors who are genuinely interested, not just available. Reputation is portable and verified.
From our founder
Why I’m building Heart Bridge Health
I grew up in Dorrigo. If you don’t know it, it’s a small town on the edge of the New England plateau in NSW — cattle, waterfalls, one main street, and a long way from anywhere with a big hospital.
My cousin was born with congenital heart disease. As a kid I didn’t really grasp how precarious that was. What I understood later is that he’s still here because of a handful of people who happened to be where he needed them: the town GP who knew his history and caught the things that mattered, the Royal Flying Doctor Service, and the hospital staff who took over when the distance would otherwise have decided things.
He’s 37 now. He’s built a career, a life, the kind of relationships that hold people up. He’s given more to the people around him than I could fit in a post.
None of that happens without a doctor in the room.
That’s the part of rural healthcare people outside it don’t always see. It isn’t abstract. It comes down to whether there’s someone there on the day it counts. Too many Australian towns are running short, and the doctors who would happily work in them.. a lot of them international medical graduates still trying to find their footing here… get lost in a system that makes it far harder than it should be.
That’s what I’m building Heart Bridge Health to change. Getting good doctors to the communities that need them, without the friction in between.
For my cousin, someone was there. I’d like that to be true for a great many more people.
#IMG #ruralhealthcare
Jade Gulliver — Founder & Director
Australia’s direct GP marketplace. No agency fees, no middleman.
Connecting doctors and clinics directly — the app is live on iOS and Android.